1. Introduction
Testosterone is a physiologically relevant androgen in women, produced by the ovaries, adrenal glands, and peripheral conversion of steroid precursors.1 Although historically perceived as predominantly a male hormone, testosterone contributes to female sexual function and several broader physiological processes.1,2
The most established evidence-based indication for testosterone therapy in women is the treatment of hypoactive sexual desire disorder (HSDD) in carefully selected postmenopausal women.2–4 International consensus statements and clinical practice guidelines acknowledge that appropriately dosed testosterone therapy may improve sexual desire and related aspects of sexual function in this population, while emphasizing the importance of maintaining physiologic dosing and avoiding supraphysiologic exposure.2,4
More recently, alternative administration strategies, including short-term and on-demand testosterone approaches, have also been explored in selected populations, although safety data remain limited and heterogeneous.5
Despite these recommendations, important uncertainties remain regarding the long-term safety of testosterone therapy in women, particularly when non-standardized, compounded, or prolonged-delivery formulations are used. Testosterone pellets have gained attention in some clinical settings because of their convenience and sustained hormone delivery. However, concerns persist regarding dose variability, prolonged systemic exposure, limited reversibility once pellets have been implanted, and the potential for supraphysiologic serum testosterone concentrations.2–4
Serious adverse events attributed to testosterone therapy in women are frequently discussed in clinical and public discourse, yet the extent to which such concerns are supported by peer-reviewed case-based evidence remains unclear. While case reports do not establish incidence or causality, they remain valuable for the early detection of rare or unexpected safety signals and for generating clinically relevant hypotheses regarding potential harm.6,7
Given the ongoing debate regarding the safety of subcutaneous testosterone pellet therapy in women, this review aimed to systematically identify and critically examine published case reports describing serious adverse events potentially associated with this intervention.
2. Methods
2.1. Review Design
This was a structured narrative review of published case reports describing serious adverse events potentially associated with subcutaneous testosterone pellet therapy in women. The study identification, screening, eligibility assessment, and selection process were conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement.8 Given the descriptive nature of case-based evidence, clinical heterogeneity of the adverse events, and the small number of eligible reports, findings were synthesized narratively rather than quantitatively.
2.2. Search Strategy
A structured literature search was conducted to identify published case reports describing adverse events potentially associated with subcutaneous testosterone pellet therapy in women. The electronic databases PubMed/MEDLINE, Embase, Scopus, and Web of Science were systematically searched from inception to May 12, 2026.
The search strategy was specifically designed to identify case-based reports involving subcutaneous testosterone pellet therapy, combining terms related to testosterone pellets, testosterone implants, and subcutaneous testosterone, along with filters or equivalent search terms for case reports. Complete database-specific search strategies are provided in Supplementary Table S1.
Given the exploratory pharmacovigilance-oriented objective of this review, case reports were intentionally selected as the primary evidence source because they provide individualized clinical descriptions of uncommon or serious adverse events, allowing assessment of temporal association, clinical evolution, alternative explanations, and potential causal plausibility.
2.3. Search Sensitivity Analysis
To enhance sensitivity and minimize the risk of missing relevant reports due to indexing limitations of the automatic case report filter, an additional search was performed in PubMed/MEDLINE on June 13, 2026, without using the case reports filter. Free-text terms for study design (“case report”, “case reports”, “case series”) and broader exposure terms (“testosterone therapy”, “androgen therapy”, “testosterone replacement therapy”) were added to the original strategy. This supplementary search did not identify any additional eligible case reports (Supplementary Table S2).
2.4. Eligibility Criteria
A serious adverse event (SAE) was defined according to the International Council for Harmonisation (ICH) E2A guideline as an event resulting in death, life-threatening illness, hospitalization, persistent disability, or another medically important outcome.9 Eligible publications were case reports describing women exposed to subcutaneous testosterone pellet therapy in whom a reported SAE was considered potentially associated with the intervention.
Studies were excluded if they involved male participants; did not include exposure to subcutaneous testosterone pellets; failed to describe an individualized SAE; lacked sufficient clinical detail to establish at least a plausible temporal relationship between testosterone exposure and the reported outcome; or consisted of review articles, editorials, conference abstracts without adequate case-level information, or other non–case-based publications.
2.5. Study Selection
Study selection was conducted independently by the two authors in a two-stage screening process.
First, titles and abstracts of all retrieved records were screened for potential eligibility. Full texts were subsequently obtained and assessed for studies considered potentially relevant after initial screening. Discrepancies regarding eligibility were resolved through discussion and consensus.
2.6. Data Extraction
For each included case report, data were extracted using a standardized approach, including author and year of publication, patient age and relevant clinical characteristics, indication for testosterone therapy (when reported), testosterone formulation, dose and duration of exposure, reported serum testosterone concentrations (when available), characteristics of the adverse event, relevant comorbidities or potential confounding risk factors, management of the adverse event, clinical outcome and follow-up, and the authors’ interpretation regarding possible causal association. Given the expected clinical heterogeneity and the inherently descriptive nature of case-based evidence, findings were synthesized narratively rather than quantitatively.
2.7. Methodological Quality Appraisal
Methodological reporting quality of the included case reports was assessed using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Case Reports,10 which evaluates completeness and transparency across eight domains, including patient description, clinical history, diagnostic assessment, intervention details, outcomes, adverse event reporting, and clinical lessons. Given the nature of case report evidence, this appraisal was intended to assess reporting quality and methodological completeness rather than formal comparative risk of bias.
2.8. Data Synthesis and Analytical Approach
Given the small number of eligible reports, clinical heterogeneity of the adverse events, and the descriptive nature of case-based evidence, quantitative synthesis, incidence estimation, and formal causal inference were not attempted. Instead, this review adopted a case-based translational evidence synthesis approach, integrating individual clinical observations with broader pharmacovigilance and clinical safety considerations. The objective was not to estimate event frequency, but rather to examine the availability, characteristics, and interpretive value of published serious adverse event reports involving testosterone pellet therapy in women.
3. Results
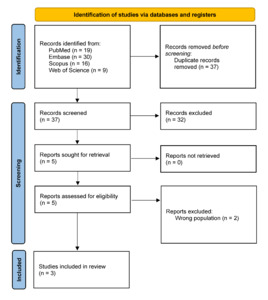
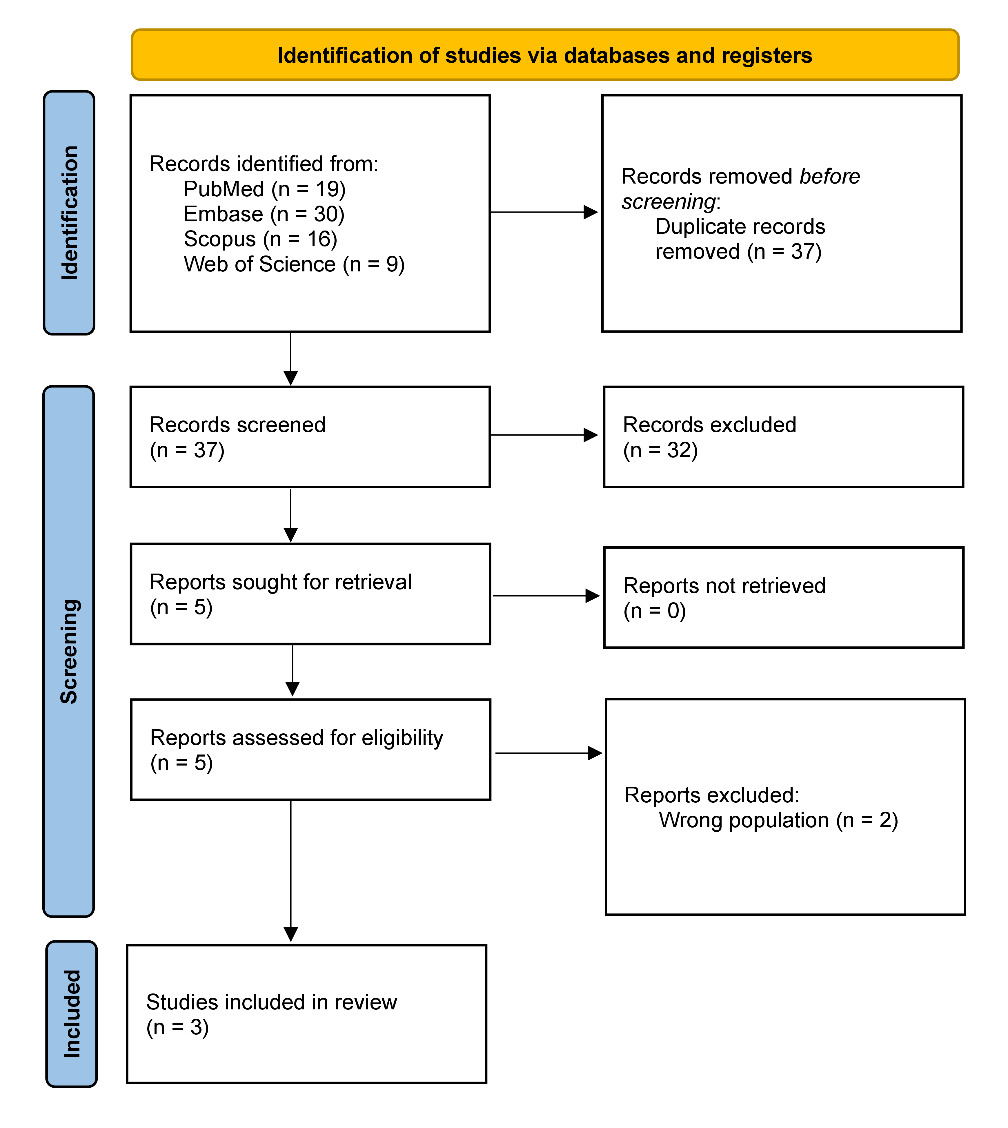
The structured literature search across PubMed, Embase, Scopus, and Web of Science identified a total of 74 records. After removal of 37 duplicate records, 37 unique records remained for title and abstract screening. Following initial screening, five case reports were considered potentially eligible for full-text assessment. Of these, two were excluded for failing to meet the predefined eligibility criteria, and three case reports were ultimately included in the review for describing adverse events potentially associated with subcutaneous testosterone pellet therapy in women (Figure 1). A supplementary search in PubMed without the automatic case-report filter and with additional free-text terms for study design and exposure identified no further eligible case reports. The excluded full-text studies and the corresponding reasons for exclusion are detailed in Supplementary Table S3.
3.1. Characteristics of Included Case Reports
The three included case reports described clinically distinct serious adverse events reported in peri- or postmenopausal women receiving subcutaneous testosterone pellet therapy.11–13 Reported events included non-arteritic cilioretinal artery occlusion, severe psychiatric manifestations occurring in the context of markedly elevated serum testosterone concentrations after prolonged pellet use, and portomesenteric venous thrombosis in a postmenopausal woman with multiple pre-existing thrombotic risk factors.11–13 The interval between testosterone exposure and event presentation ranged from 1 month to more than 10 years, and supraphysiologic testosterone concentrations were documented in two reports. Relevant coexisting clinical factors included retinal migraine, obesity, chronic obstructive pulmonary disease, elevated hematocrit, and a personal or family history of psychiatric disorders. Detailed clinical characteristics of the included case reports are summarized in Table 1. Considerations regarding temporal relationships, potential confounding factors, dechallenge/rechallenge findings, and overall interpretation of the reported events are presented in Supplementary Table S4.
3.2. Methodological Quality Assessment
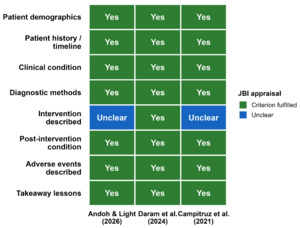
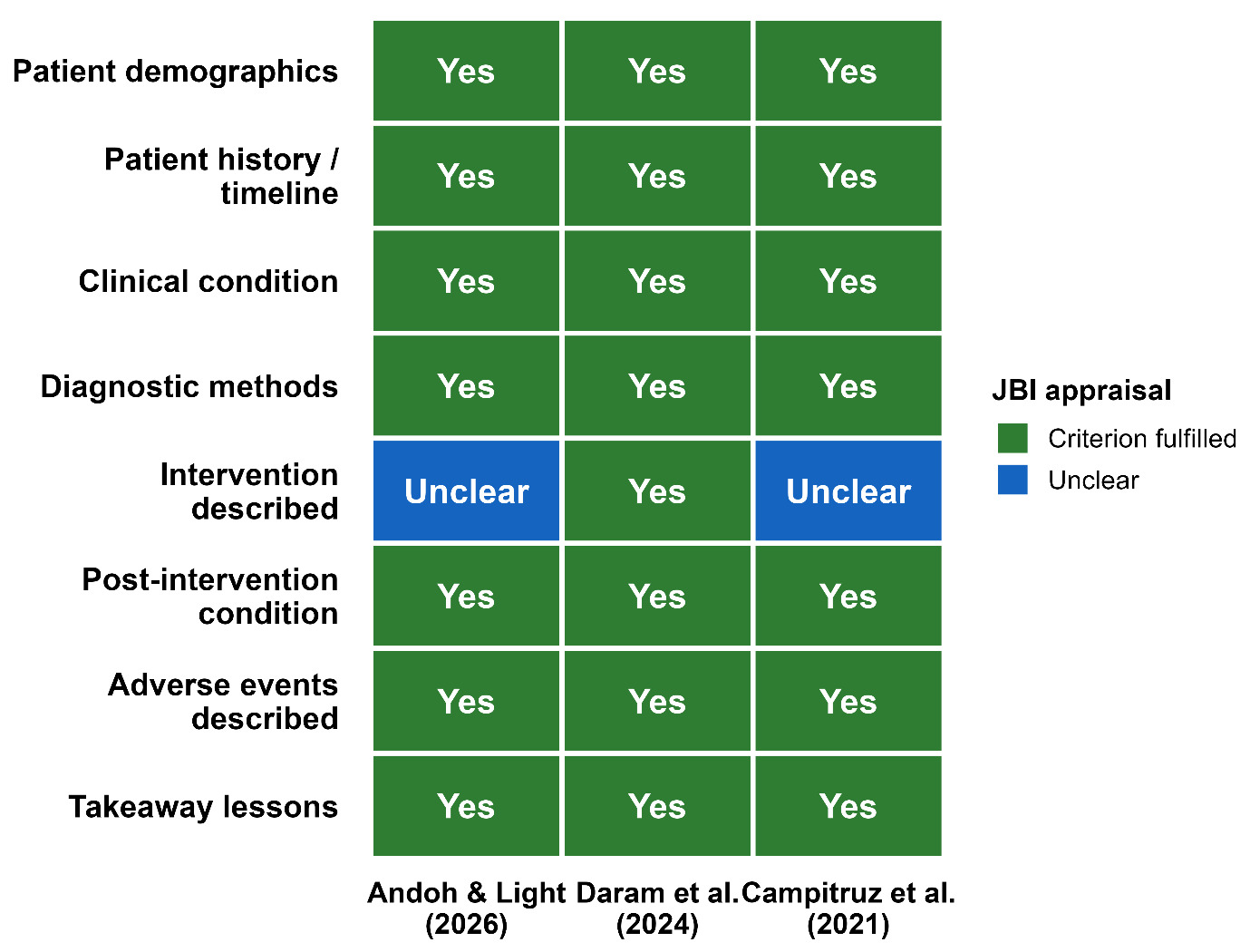
Methodological reporting quality of the included case reports was assessed using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Case Reports,10 a standardized tool designed to evaluate the completeness and transparency of case report reporting across eight domains, including patient characteristics, clinical history, diagnostic assessment, intervention, outcomes, adverse events, and key clinical lessons. Most appraisal criteria were fulfilled across the included reports (Figure 2). Two reports were rated as unclear for the intervention-description domain because details regarding the testosterone pellet formulation and administration were incompletely reported. Item-level JBI judgments and supporting rationale for each assessment are presented in Supplementary Table S5.
4. Discussion
The principal finding of this review was the identification of only three peer-reviewed case reports directly describing adverse events potentially associated with subcutaneous testosterone pellet therapy in women.11–13 These reports involved clinically significant but heterogeneous events, including non-arteritic cilioretinal artery occlusion, severe psychiatric manifestations, and portomesenteric venous thrombosis. While these events raise legitimate safety concerns, interpretation of causality requires caution.
In the ophthalmologic case, the patient had a prior history of retinal migraine, although extensive systemic evaluation did not identify thrombophilia or another clear alternative etiology.11 In the psychiatric case, the presence of markedly elevated testosterone concentrations, prolonged exposure, dose escalation, and recurrence after re-exposure strengthen the plausibility of a causal relationship, although this scenario may represent supraphysiologic exposure rather than monitored physiologic replacement.12 In the thrombotic case, the authors acknowledged concomitant prothrombotic risk factors, including obesity, chronic obstructive pulmonary disease, elevated hematocrit, and possible chronic hypoxia.13
Taken together, these reports suggest possible safety signals, but they do not establish definitive causality. Their primary value lies in hypothesis generation and clinical vigilance rather than causal inference.14
4.1. Regulatory and Clinical Context
Testosterone therapy in women remains an area of ongoing clinical and regulatory debate. Although testosterone has demonstrated therapeutic benefit in selected clinical contexts, particularly for postmenopausal women with hypoactive sexual desire disorder, concerns remain regarding long-term safety, appropriate dosing, and formulation selection.2–4
A key distinction must be made between physiologic therapeutic use and supraphysiologic, poorly monitored, compounded, or non-standardized use. This distinction is especially relevant for pellet formulations, which may be associated with prolonged exposure, limited reversibility once implanted, and increased risk of achieving supraphysiologic serum testosterone levels. The psychiatric case identified in this review particularly illustrates this concern, as testosterone concentrations substantially exceeded expected physiologic female ranges.12
Current clinical recommendations for testosterone therapy in women are limited to carefully selected postmenopausal women with hypoactive sexual desire disorder and are intended to achieve physiologic testosterone concentrations. Both the Global Consensus Position Statement2 and the ISSWSH Clinical Practice Guideline4 caution against testosterone pellet therapy when it produces supraphysiologic exposure or cannot be adequately titrated after implantation. More specifically, the Global Consensus Position Statement excludes pellets and other supraphysiologic formulations from its physiologic-dose recommendations, while the ISSWSH guideline states that pellets are not recommended because implants may produce supraphysiologic concentrations and do not permit dose titration. These concerns apply specifically to pellet formulations and should be distinguished from compounded testosterone preparations in general, which may or may not share the same pharmacokinetic limitations. However, despite these theoretical concerns, published reports of serious adverse events associated with testosterone pellet therapy in women remain scarce. In the present review, only three case reports describing such events were identified. This discrepancy between guideline caution and the limited published evidence of harm underscores the need for improved pharmacovigilance and higher-quality studies before definitive conclusions about safety can be drawn. A recent structured narrative review similarly concluded that, although testosterone pellets provide long-term delivery, most available data derive from observational studies, and both efficacy and safety remain insufficiently characterized.15
Thus, concerns raised by inappropriate, poorly monitored, or supraphysiologic pellet use should not be generalized to all evidence-based testosterone therapy in women.
4.2. Comparison with Existing Literature
The findings of the included case reports should be interpreted within the context of the broader evidence base on testosterone therapy in women. Randomized controlled trials and meta-analyses evaluating testosterone therapy for hypoactive sexual desire disorder in postmenopausal women have generally demonstrated reassuring short-term safety profiles when physiologic doses are used, with adverse effects primarily limited to acne, hirsutism, and other mild androgenic symptoms, while serious adverse events remain infrequently reported.2–4,16 However, these studies have predominantly evaluated transdermal formulations designed to achieve physiologic testosterone concentrations and allow dose titration or treatment discontinuation when necessary. In contrast, testosterone pellet therapy provides prolonged hormone exposure over several months and may result in supraphysiologic testosterone concentrations, with limited ability to modify or reverse exposure once implanted. Consequently, the serious adverse events described in the present review may not be representative of the safety profile observed with physiologically dosed testosterone therapy using titratable formulations. This distinction highlights an important evidence gap, as long-term safety data for pellet therapy remain limited and uncommon serious adverse events may be underrecognized, underreported, or insufficiently characterized in the existing literature.4,15
4.3. Clinical Implications
Case reports remain an important component of pharmacovigilance, particularly for rare or unexpected adverse events. However, attribution of harm to hormonal interventions requires careful interpretation. Meaningful assessment of potential causality depends on adequate documentation of clinical indication, dose, formulation, serum hormone concentrations, duration of exposure, coexisting risk factors, concomitant medications, diagnostic exclusion of alternative causes, clinical evolution after discontinuation, and, when applicable, recurrence after re-exposure.6,7,11–13
Without such detail, isolated anecdotal observations cannot meaningfully inform risk estimation or clinical decision-making. Clinicians considering testosterone pellet therapy should therefore ensure careful patient selection, risk assessment, dose monitoring, and counseling regarding uncertainties in long-term safety.
4.4. Strengths and Limitations
This review has several strengths, including a structured multi-database search, explicit eligibility criteria, a supplementary sensitivity search using broader exposure and case-report terms, and methodological appraisal of included reports using the Joanna Briggs Institute critical appraisal framework.10 However, important limitations should be acknowledged. First, the analysis was restricted to published case reports, which represent a low level of evidence and are inherently vulnerable to publication bias, incomplete reporting, and uncertain causal attribution. Second, the small number of included reports precludes meaningful generalization regarding incidence, frequency, comparative safety, or the overall risk profile of testosterone pellet therapy in women. Third, spontaneous pharmacovigilance databases, regulatory adverse-event reporting systems, observational studies, and randomized clinical trial safety datasets were not systematically analyzed. Although multiple databases were searched, relevant cases may still have been missed if they were not indexed as case reports or did not use pellet-specific terminology. Therefore, the identification of only three published case reports should not be interpreted as evidence that such events are rare, or as evidence of safety or absence of harm, since underreporting, publication bias, variable clinical recognition, and use of testosterone pellets outside academic settings may all influence the number of cases available in the literature.
4.5. Future Research Directions
The current evidence base underscores the need for more systematic safety evaluation of testosterone pellet therapy in women. Prospective registries, pharmacovigilance analyses, multicenter observational cohorts, and better characterization of dose-response relationships would substantially improve understanding of rare but clinically important adverse events. More transparent reporting of suspected complications would also facilitate more balanced evidence-based regulatory and clinical decision-making.
5. Conclusion
The limited number of peer-reviewed case reports identified in this review should not be interpreted as evidence of safety, nor as proof of absence of clinically important risk. Rather, the available literature suggests that serious adverse events may occur under certain circumstances, particularly in the context of supraphysiologic exposure or concomitant risk factors, but remains insufficient to define the true magnitude of risk. Strengthening pharmacovigilance, improving transparency in adverse event reporting, and generating higher-quality safety evidence should be priorities for future research.
Conflict of Interest / Competing Interests
The authors declare no conflicts of interest relevant to this work.
Ethics Approval and Consent
This review was based exclusively on previously published literature and did not involve the collection of new data from human participants or animals. Ethical approval and informed consent were therefore not required for this study.
AI Tool Use Disclosure
Artificial intelligence tools were used for language editing and formatting only. All scientific content, interpretations, references, and conclusions were reviewed and verified by the authors, who accept full responsibility for the final manuscript.
Third-Party Material Permissions
No third-party material requiring permission has been reproduced in this manuscript. The tables and figures were created by the authors based on the data and methods described in the cited sources.
Data Availability
All data analyzed in this review were obtained from previously published sources. The extracted data supporting the findings are presented in the article and its supplementary material.
Funding
This research received no external funding.
Reporting Guidelines
The literature search and study-selection process were reported in accordance with the applicable items of the PRISMA 2020 statement.
Preprint Disclosure
This manuscript has not been posted as a preprint and has not been previously published.
Author Contributions (CRediT)
Conceptualization: Lucas Caseri Câmara (Lead). Data curation: Lucas Caseri Câmara (Supporting), Matheus Hissa Lourenço Ferreira (Lead). Methodology: Lucas Caseri Câmara (Equal), Matheus Hissa Lourenço Ferreira (Equal). Supervision: Lucas Caseri Câmara (Lead). Writing – original draft: Lucas Caseri Câmara (Equal), Matheus Hissa Lourenço Ferreira (Equal). Writing – review & editing: Lucas Caseri Câmara (Equal), Matheus Hissa Lourenço Ferreira (Equal). Validation: Matheus Hissa Lourenço Ferreira (Equal). Visualization: Matheus Hissa Lourenço Ferreira (Equal).
Abbreviations
HSDD, hypoactive sexual desire disorder; ICH, International Council for Harmonisation; JBI, Joanna Briggs Institute; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; SAE, serious adverse event.